If you or someone you love has been diagnosed with hormone receptor-positive breast cancer, which accounts for about 70-80% of all breast cancers, you’ve likely heard two names come up constantly in doctor’s offices: Tamoxifen and Aromatase Inhibitors. These aren’t just pills; they are the backbone of modern cancer care, designed to stop cancer cells from getting the fuel they need to grow. But picking between them isn’t a simple choice. It depends heavily on whether you are premenopausal or postmenopausal, your risk of recurrence, and how your body handles specific side effects.
This guide cuts through the medical jargon to explain exactly how these drugs work, who they are best for, and what real life looks like while taking them. We’ll look at the hard data from major clinical trials and the lived experiences of patients to help you have a more informed conversation with your oncologist.
How Hormone Therapy Actually Works
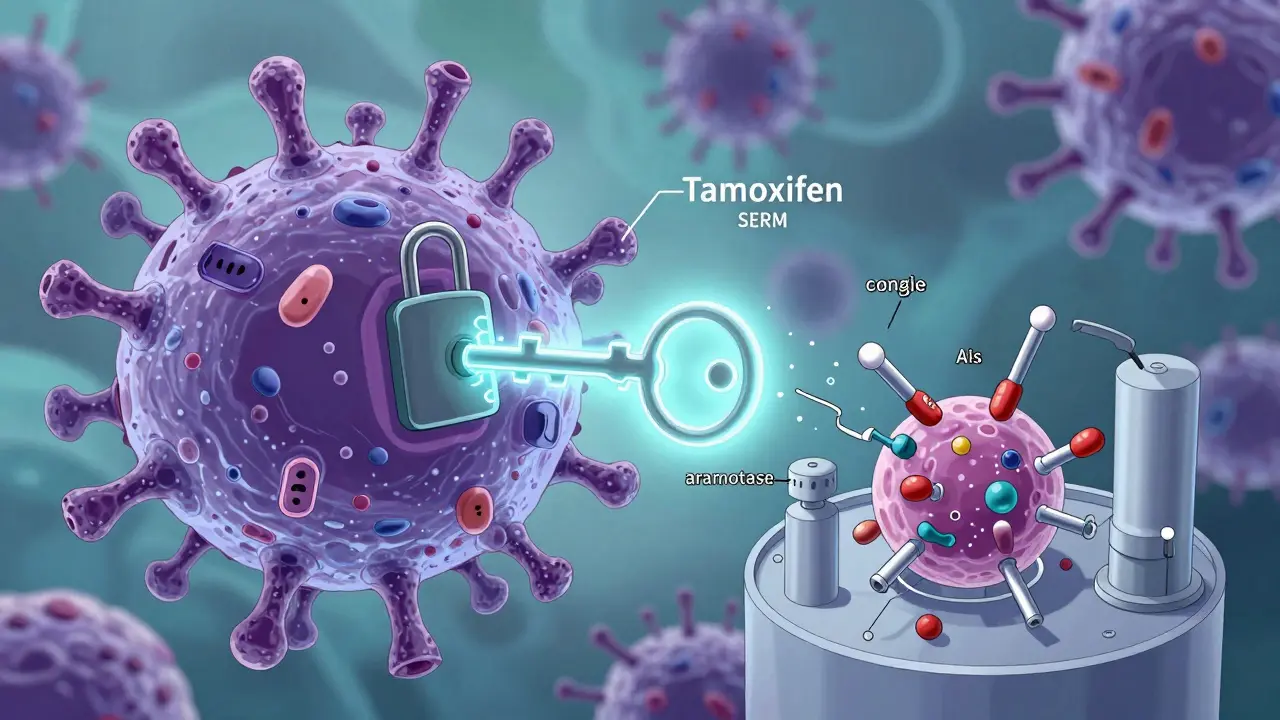
To understand why we use these drugs, we first need to understand the enemy. Hormone receptor-positive (HR+) breast cancer cells have receptors on their surface that act like locks. Estrogen, a natural hormone, acts like the key. When estrogen fits into those locks, it tells the cancer cell to divide and grow. Hormone therapy doesn’t kill the cancer directly like chemotherapy does. Instead, it starves it.
Tamoxifen is a type of drug called a Selective Estrogen Receptor Modulator (SERM). Think of Tamoxifen as a fake key. It jams into the lock on the cancer cell, preventing the real estrogen key from entering. The cell gets no signal to grow. This works well because Tamoxifen blocks estrogen in breast tissue but can actually have protective effects on other parts of the body, like bones and the heart, depending on your age.
Aromatase Inhibitors (AIs), on the other hand, take a different approach. They don’t block the lock; they destroy the key factory. In postmenopausal women, most estrogen is made by an enzyme called aromatase, which converts other hormones into estrogen in fat tissue, muscles, and skin. AIs shut down this enzyme. Without aromatase, your body produces almost no new estrogen. Third-generation AIs like anastrozole, letrozole, and exemestane can reduce estrogen levels by 95-98%. This makes them incredibly potent, but also means they affect the whole body’s estrogen balance.
The Menopause Factor: Why Status Matters
Your menopausal status is the single biggest factor in choosing between Tamoxifen and AIs. This isn’t just a preference; it’s biology.
For postmenopausal women, whose ovaries have stopped producing estrogen, AIs are generally the standard first-line treatment. Major studies, including the ATAC trial and updates from the Early Breast Cancer Trialists' Collaborative Group (EBCTCG), show that AIs reduce the risk of cancer coming back by about 30% compared to Tamoxifen during the treatment period. If you are past menopause, your body relies on peripheral conversion for estrogen, making AIs highly effective.
For premenopausal women, the story is different. Your ovaries are still churning out massive amounts of estrogen. If you take an AI, your brain senses the low estrogen and signals the ovaries to produce even more, effectively overriding the drug. That’s why AIs alone don’t work for premenopausal women. To use an AI in this group, you must combine it with Ovarian Function Suppression (OFS)-usually injections like goserelin (Zoladex) that temporarily shut down the ovaries. Even then, recent trials like TEXT and SOFT show that while OFS plus an AI is slightly better than OFS plus Tamoxifen for high-risk patients, Tamoxifen remains a very strong option, especially for lower-risk cases.
| Feature | Tamoxifen | Aromatase Inhibitors (Anastrozole/Letrozole) |
|---|---|---|
| Mechanism | Blocks estrogen receptors (fake key) | Stops estrogen production (destroys factory) |
| Best For | Premenopausal women; some postmenopausal | Postmenopausal women |
| Bone Health | Protects bone density | Increases risk of osteoporosis/fractures |
| Joint Pain | Less common | Very common (up to 50% of users) |
| Uterine Risk | Slightly increases endometrial cancer risk | No increased uterine risk |
| Blood Clots | Higher risk of DVT/PE | Lower risk |
Efficacy: What Do the Numbers Say?
When it comes to stopping cancer from returning, both drugs are powerful, but AIs often edge out Tamoxifen in head-to-head comparisons for postmenopausal women. The EBCTCG meta-analysis, which looked at over 31,000 women, found that after 10 years, breast cancer mortality was lower with AIs (12.1%) than with Tamoxifen (14.2%). That’s a significant difference.
However, "better" isn’t always the right word if the side effects make the treatment unbearable. The benefit of AIs is most pronounced in the first 4-5 years of treatment. After that, the curves flatten out. For many women, especially those with early-stage, low-risk cancer, Tamoxifen offers a very robust protection with a side effect profile that might be easier to manage long-term.
For premenopausal women, the TEXT and SOFT trials showed that adding exemestane (an AI) to ovarian suppression reduced 5-year recurrence risk to 6.9%, compared to 10.1% with Tamoxifen plus suppression. That’s an absolute reduction of 3.2%. While statistically significant, it means that for every 31 women treated with the stronger regimen, one additional recurrence is prevented. Doctors weigh this against the harsh side effects of shutting down ovaries and blocking estrogen simultaneously.
Side Effects: The Real-Life Trade-Offs
Medicine textbooks list side effects, but patient forums tell the real story. Quality of life matters immensely when you’re taking a pill every day for five to ten years.
Tamoxifen’s main villains: Hot flashes and night sweats are extremely common, affecting up to 60-70% of users. Many describe them as worse than natural menopause. There’s also a small but serious risk of blood clots (deep vein thrombosis or pulmonary embolism) and a slight increase in the risk of endometrial (uterine) cancer. Women on Tamoxifen need to report any unusual vaginal bleeding immediately. On the flip side, Tamoxifen tends to preserve bone density and may offer cardiovascular benefits in younger women.
Aromatase Inhibitors’ main villains: Joint pain and stiffness (arthralgia) are the biggest complaints. Up to half of women on AIs report moderate to severe joint pain, which can limit mobility and sleep. Fatigue and "chemo brain" (cognitive fog) are also frequently reported. Because AIs strip away estrogen so aggressively, they accelerate bone loss, increasing the risk of osteoporosis and fractures. However, they do not carry the same risks of blood clots or uterine cancer as Tamoxifen.
Data from patient registries shows that about 31% of women prescribed AIs eventually need to switch doses or stop treatment due to side effects, compared to about 19% for Tamoxifen. This is a crucial point: if you can’t tolerate the drug, it won’t help you. Adherence is key.
Duration of Treatment: 5 Years or More?
The standard course for both Tamoxifen and AIs is five years. But for many women, doctors now recommend extending treatment to seven or ten years. Studies like MA.17R and DATA show that continuing therapy beyond five years further reduces the risk of late recurrences, particularly for women with larger tumors or positive lymph nodes.
However, longer treatment means longer exposure to side effects. The decision to extend is highly personalized. Newer research, such as the PERSEPHONE trial, is even looking at whether three years of Tamoxifen is enough for very low-risk patients. Currently, genomic tests like Oncotype DX or Prosigna help doctors estimate your individual risk of recurrence, guiding whether you need chemotherapy, extended hormone therapy, or just the standard five years.
Managing Side Effects: You Don't Have to Suffer in Silence
If you are struggling with side effects, talk to your care team. There are strategies to help:
- For Joint Pain (AIs): Regular low-impact exercise like swimming or walking can significantly reduce stiffness. Some doctors prescribe duloxetine (Cymbalta), which has been shown to help with AI-induced arthralgia. Vitamin D and calcium supplements are essential to protect bones.
- For Bone Loss: If you are on an AI, you should have a DEXA scan to check bone density. If your bones are weakening, medications like zoledronic acid or denosumab can strengthen them and prevent fractures.
- For Hot Flashes (Tamoxifen): Non-hormonal options like certain antidepressants (venlafaxine) or gabapentin can help. Avoiding triggers like spicy food, alcohol, and hot environments also helps.
- Switching Drugs: If one drug is too hard to tolerate, switching is an option. Some women start with Tamoxifen for two to three years and then switch to an AI for the remaining time. The OBSERVATION registry suggests this "sequential" approach offers similar outcomes to starting with an AI upfront, with potentially fewer early side effects.
Cost and Access Considerations
In countries with universal healthcare or good insurance coverage, cost shouldn’t be the primary driver. However, globally, Tamoxifen is much cheaper. Generic Tamoxifen costs around $15 per month, while branded AIs can cost upwards of $150 per month. In low-resource settings, Tamoxifen remains the only feasible option for many. In North America and Europe, both are widely accessible, but prior authorizations for AIs can sometimes cause delays. Always check with your pharmacist about generic versions of AIs, which are now available and significantly cheaper.
Future Directions: Beyond Tamoxifen and AIs
Science never stops. For women whose cancer returns despite being on AIs, new drugs called Selective Estrogen Receptor Degraders (SERDs) are changing the game. Elacestrant and camizestrant are oral SERDs that destroy the estrogen receptor entirely rather than just blocking it. Early trials show promise, especially for tumors with specific genetic mutations (ESR1). While these aren’t yet first-line treatments for early-stage cancer, they represent the next evolution in hormone therapy.
Personalized medicine is also advancing. Pharmacogenomic testing, which looks at genes like CYP2D6, can predict how well your body will convert Tamoxifen into its active form. If you are a "poor metabolizer," Tamoxifen might be less effective for you, and your doctor might lean toward an AI (if postmenopausal) or consider other options.
Can I take Tamoxifen and an Aromatase Inhibitor at the same time?
Generally, no. Taking them together is not recommended because Tamoxifen can interfere with the effectiveness of Aromatase Inhibitors. They work through different mechanisms, and combining them hasn’t shown added benefit in clinical trials. Doctors usually prescribe one or the other, or sequentially (one after the other).
Which drug is better for preventing osteoporosis?
Tamoxifen is better for bone health. It acts like estrogen on bone tissue, helping to maintain density. Aromatase Inhibitors, by stripping away estrogen, accelerate bone loss and increase fracture risk. If you already have osteoporosis, Tamoxifen might be the preferred choice unless your cancer risk is very high.
Do I need to change my diet while on hormone therapy?
While no specific "cancer diet" is mandated, maintaining a healthy weight is crucial. Fat tissue produces estrogen, so excess weight can counteract the effects of Aromatase Inhibitors. A balanced diet rich in vegetables, fruits, and whole grains, along with regular exercise, supports overall health and helps manage side effects like fatigue and joint pain.
What if I experience vaginal bleeding while on Tamoxifen?
Any unusual vaginal bleeding, spotting, or discharge while taking Tamoxifen should be reported to your doctor immediately. Although the risk is small, Tamoxifen slightly increases the chance of endometrial hyperplasia or cancer. Prompt evaluation allows for early detection and treatment if necessary.
Can I drink alcohol while taking these medications?
Moderate alcohol consumption is generally considered safe, but excessive drinking can raise estrogen levels and increase the risk of cancer recurrence. It can also worsen liver function, as both Tamoxifen and AIs are processed by the liver. Most oncologists recommend limiting alcohol to occasional, moderate intake.