Stimulant Cardiac Risk Assessment Tool
Patient Profile & Health History
Current Status
Complete the form to see your preliminary risk assessment.
Recommendations & Next Steps
Disclaimer: This tool is for educational purposes only and does not constitute medical advice. It is based on general guidelines from organizations like the AAP and AHA. Always consult a qualified healthcare provider before starting or changing medication. If you experience chest pain, fainting, or severe palpitations, seek emergency care immediately.
For millions of people managing Attention-Deficit/Hyperactivity Disorder (ADHD), a neurodevelopmental condition characterized by persistent patterns of inattention, hyperactivity, and impulsivity that interfere with functioning or development, prescription stimulants are often the most effective tool available. These medications help focus the mind and regulate behavior. However, because these drugs affect the central nervous system, they also impact the cardiovascular system. This raises a critical question for patients and doctors alike: do stimulant medications, such as amphetamines and methylphenidate, increase the risk of dangerous heart rhythm disturbances known as cardiac arrhythmias?
The short answer is nuanced. For most healthy individuals, the risk is low. But for those with underlying heart conditions or specific genetic factors, the stakes are higher. Understanding this balance requires looking beyond simple yes-or-no answers to examine how these drugs work, who is at risk, and what safer alternatives exist.
How Stimulants Affect the Heart
To understand the risk, we first need to look at the mechanism. Stimulant medications like Adderall (mixed amphetamine salts), a central nervous system stimulant used to treat ADHD and narcolepsy, Ritalin (methylphenidate), a CNS stimulant primarily used to treat ADHD and narcolepsy, and Vyvanse (lisdexamfetamine), a prodrug of dextroamphetamine used for ADHD and binge eating disorder work by increasing the levels of dopamine and norepinephrine in the brain. Norepinephrine is not just a neurotransmitter; it is also a hormone that signals the body’s "fight or flight" response.
When you take a stimulant, your body reacts slightly as if it is under stress. According to data from CHADD (Children and Adults with Attention-Deficit/Hyperactivity Disorder), published in 2023, typical prescription doses cause modest increases in vital signs. Most patients see an increase in heart rate of about 1 to 2 beats per minute and a slight rise in blood pressure-systolic pressure goes up by 1 to 4 mmHg, and diastolic by 1 to 2 mmHg. For a healthy heart, this is usually negligible. Think of it like walking up a flight of stairs; your heart works a little harder, but it returns to normal quickly.
However, arrhythmias are not just about speed; they are about electrical stability. The heart relies on precise ion channels to maintain its rhythm. If these channels are disrupted, the electrical signal can fire too early, too late, or chaotically. This is where the distinction between prescription drugs and illicit substances becomes starkly clear, yet relevant for understanding the biological ceiling of risk.
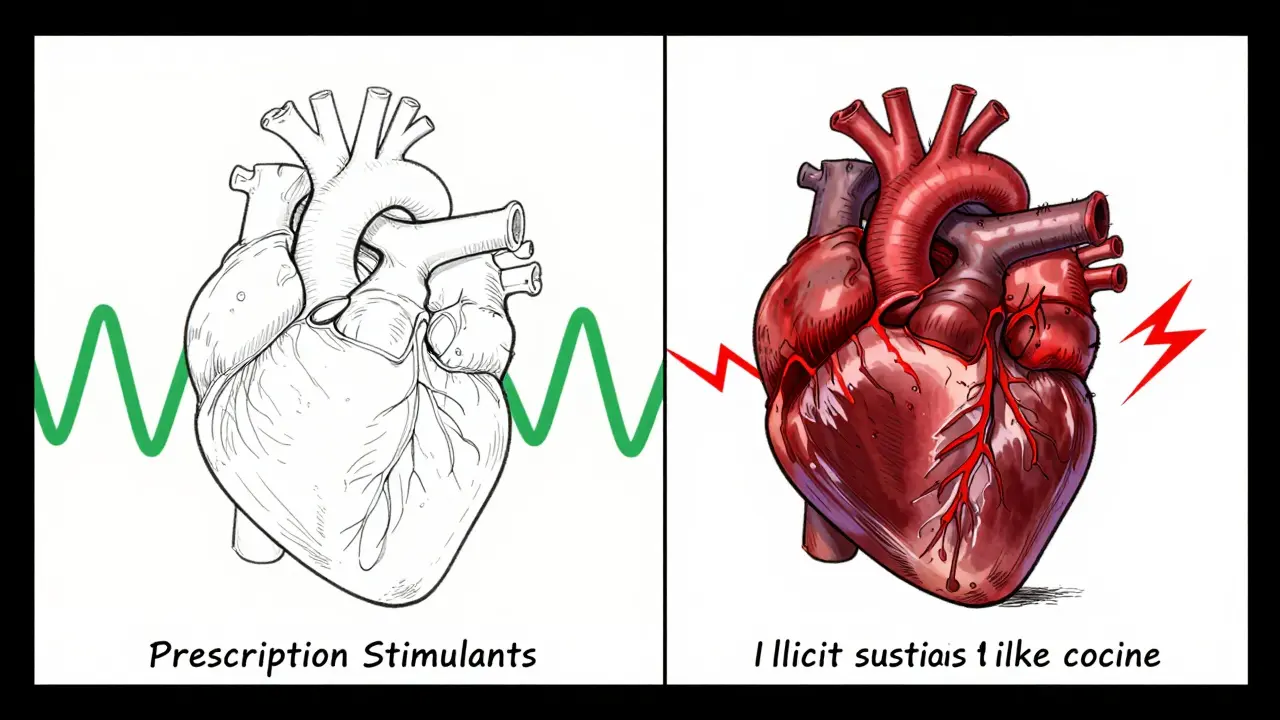
Prescription vs. Illicit Stimulants: A Risk Comparison
It is crucial to separate prescription ADHD medications from illicit stimulants like cocaine and methamphetamine when assessing risk. While they share similar mechanisms, the dose and purity differ vastly. Research published in the European Heart Journal in 2025 highlighted that chronic use of cocaine and methamphetamine induces significant electrical and structural remodeling in the heart.
Cocaine blocks voltage-dependent potassium channels and fast inward sodium channels. This prolongs the QT interval-a measure of the time it takes for the heart's ventricles to depolarize and repolarize. A prolonged QT interval is a known risk factor for Torsades de Pointes, a life-threatening arrhythmia. Methamphetamine similarly inhibits transient outward potassium current and L-type calcium current. Users of these illicit drugs face a 2.5 to 4.5 times higher crude incidence of ventricular arrhythmias compared to non-users.
Prescription stimulants do not typically block these channels to the same extent at therapeutic doses. However, they do increase sympathetic tone (the activity of the sympathetic nervous system). In susceptible individuals, this increased tone can trigger arrhythmias. The key difference is that prescription drugs are taken in controlled, low doses, whereas illicit use often involves high, unpredictable doses that overwhelm the heart’s electrical system.
| Factor | Prescription Stimulants (e.g., Adderall, Ritalin) | Illicit Stimulants (Cocaine, Methamphetamine) |
|---|---|---|
| Average Heart Rate Increase | 1-2 beats per minute | Significant tachycardia (often >100 bpm) |
| Blood Pressure Impact | Slight increase (1-4 mmHg systolic) | Hypertensive crisis potential |
| Ion Channel Blockade | Minimal at therapeutic doses | Direct blockade of Na+, K+, and Ca2+ channels |
| Arrhythmia Risk Profile | Low in healthy hearts; elevated in pre-existing conditions | High risk of ventricular fibrillation and sudden death |
| Structural Heart Changes | Uncommon; mild cardiomyopathy possible long-term | Fibrosis, hypertrophy, and severe remodeling common |
Who Is at Highest Risk?
Not everyone faces the same level of danger. Age and pre-existing health conditions play a massive role in determining risk. Recent studies have shed light on specific vulnerable populations.
Older Adults: A cohort study published in PubMed Central in 2021 examined adults aged 66 and older. It found that initiating stimulant therapy was associated with a tripling of ventricular arrhythmia risk within the first 30 days (Hazard Ratio 3.0; 95% CI 1.1-8.7). Interestingly, this risk did not persist at 180 or 365 days, suggesting that the initial adjustment period is the most critical window for older patients. Overall cardiovascular event risk also increased by 40% in that first month.
Young Adults and Long-Term Use: Conversely, a March 2024 press release from the American College of Cardiology (ACC) discussed a study focusing on young adults. It noted that while the immediate risk might be lower, there is an increasing risk of cardiomyopathy over time-17% higher at one year and 57% higher at eight years. This suggests that long-term monitoring is essential even for younger patients.
Pre-existing Conditions: Individuals with congenital heart defects, hypertrophic cardiomyopathy, or long QT syndrome are at significantly higher risk. The American Academy of Pediatrics (AAP) and American Heart Association (AHA) joint statement advises caution here. If a patient has a history of unexplained sudden death in the family before age 50, or symptoms like chest pain or fainting (syncope) during exercise, stimulants may be contraindicated.
The Controversy Over ECG Screening
If the risks are real, why isn’t every patient required to have an electrocardiogram (ECG) before starting medication? This is a subject of ongoing debate among medical professionals.
In 2008, the FDA issued a public health advisory warning of a "slight increase in the chance of having heart problems." This led many clinicians to adopt routine ECG screening. However, the AAP and AHA jointly stated in 2013 that routine ECG screening is not required before starting stimulants. Their reasoning? The yield is low. Most children and young adults with ADHD do not have undetected structural heart defects that would show up on an ECG. Furthermore, delaying treatment for weeks to wait for test results can worsen educational and social outcomes.
Instead of mandatory ECGs, the current standard of care emphasizes a thorough clinical history and physical examination. Doctors look for:
- Family history of sudden cardiac death before age 50.
- Personal history of fainting spells or chest pain.
- Physical signs like abnormal heart murmurs.
Non-Stimulant Alternatives
For patients who cannot tolerate stimulants due to cardiac concerns, or for those who prefer to avoid them, non-stimulant medications offer a viable alternative. These drugs work differently, targeting norepinephrine reuptake without the direct sympathomimetic effects of amphetamines.
Atomoxetine (Strattera): This is a selective norepinephrine reuptake inhibitor. It does not cause the same spike in heart rate or blood pressure as stimulants. However, it is not entirely free of cardiac warnings. It can cause small increases in heart rate and blood pressure, so monitoring is still advised, especially in the first few weeks. Its efficacy is generally lower than stimulants, with response rates around 50-60% compared to 70-80% for stimulants.
Guanfacine (Intuniv) and Clonidine (Kapvay): These are alpha-2 adrenergic agonists. Originally designed to lower blood pressure, they actually reduce sympathetic outflow from the brain. This makes them particularly safe for patients with existing hypertension or cardiac issues. They tend to lower both heart rate and blood pressure. The downside? Sedation. Many patients report feeling tired or drowsy, which can limit their utility for daytime functioning.
Choosing an alternative depends on the individual’s profile. If blood pressure is the primary concern, guanfacine or clonidine might be ideal. If the goal is simply to avoid the "stimulant" classification while maintaining efficacy, atomoxetine is often the go-to choice.
Practical Monitoring Protocols
If you or a loved one is prescribed a stimulant, proactive monitoring is the best defense against unexpected events. Here is a practical checklist based on current guidelines:
- Baseline Check: Before starting, record your resting heart rate and blood pressure. Note any palpitations or irregular beats you already experience.
- Early Monitoring: Check vitals again within 1 to 3 months of starting the medication or changing the dose. This is when the body is adjusting.
- Ongoing Checks: Monitor blood pressure and pulse every 6 to 12 months during stable treatment.
- Red Flags: Discontinue use and seek immediate medical attention if you experience:
- Chest pain or tightness.
- Shortness of breath without exertion.
- Fainting or near-fainting episodes.
- Persistent heart rate above 100 bpm at rest.
- Irregular heartbeat sensations (palpitations).
Moving Forward: Personalized Medicine
The landscape of ADHD treatment is shifting toward personalized medicine. Researchers are currently investigating genetic markers that might predict who is susceptible to stimulant-induced arrhythmias. Polymorphisms in adrenergic receptor genes could one day allow doctors to prescribe with greater precision, avoiding trial-and-error approaches.
The American College of Cardiology is expected to release updated guidelines in late 2025 that will likely incorporate more nuanced risk stratification. Until then, the consensus remains: for the vast majority of patients, the benefits of effective ADHD treatment far outweigh the low absolute risk of serious cardiac events. As Dr. Pauline Gerard, lead author of the 2024 ACC study, noted, "The risk of that is very low... it is not a reason to stop prescribing these medications." However, "very low" is not zero. Vigilance, open communication with your healthcare provider, and regular monitoring are essential to staying safe.
Do all ADHD medications cause heart problems?
No. Not all ADHD medications carry the same cardiac risks. Stimulants like Adderall and Ritalin have a higher potential to affect heart rate and blood pressure compared to non-stimulants like Strattera (atomoxetine) or Intuniv (guanfacine). Non-stimulants are often preferred for patients with pre-existing heart conditions.
Is an ECG required before starting ADHD medication?
Currently, major organizations like the AAP and AHA do not recommend routine ECG screening for all patients. Instead, they emphasize a detailed personal and family medical history. An ECG is only recommended if red flags are identified, such as a family history of sudden cardiac death or symptoms like fainting.
Can I take stimulants if I have high blood pressure?
It depends on the severity and control of your hypertension. Stimulants can raise blood pressure slightly. If your blood pressure is well-controlled with medication, stimulants may be used with careful monitoring. However, if you have uncontrolled hypertension, non-stimulant options like guanfacine may be safer choices.
What are the signs of a dangerous heart rhythm while on stimulants?
Warning signs include chest pain, shortness of breath, fainting (syncope), or persistent palpitations (a feeling that your heart is racing or skipping beats). If you experience any of these symptoms, stop taking the medication and seek immediate medical attention.
Are older adults at higher risk for arrhythmias from ADHD meds?
Yes. Studies suggest that adults aged 66 and older face a higher risk of ventricular arrhythmias, particularly within the first 30 days of starting stimulant therapy. Close monitoring is essential for this demographic.
How do illicit stimulants compare to prescription ones regarding heart risk?
Illicit stimulants like cocaine and methamphetamine pose a significantly higher risk. They directly block cardiac ion channels and cause severe structural changes to the heart, leading to a much higher incidence of fatal arrhythmias compared to controlled prescription doses.
What should I monitor while taking ADHD stimulants?
You should monitor your resting heart rate and blood pressure regularly. Check these metrics at baseline, within 1-3 months of starting or changing dosage, and every 6-12 months thereafter. Keep a log of any unusual symptoms like dizziness or rapid heartbeat.
Are there genetic tests for stimulant heart risk?
Currently, there are no widely available commercial genetic tests specifically for predicting stimulant-induced arrhythmias. However, research into polymorphisms in adrenergic receptor genes is ongoing, which may lead to personalized testing options in the future.
13 Comments
the risk is not just about the pill its about the system pushing these drugs on kids without proper screening in my country we see many cases of undiagnosed heart issues because doctors are too busy to check properly you need to demand better care
One must consider the existential weight of such pharmacological interventions 🧠✨ The heart, that pulsating drum of life, is subjected to artificial rhythms which may disrupt the natural harmony of the soul and body alike. It is a fascinating yet terrifying prospect that we alter our very essence with such casual disregard for the ancient wisdom of physiological balance. The pretension of modern medicine often overlooks the subtle whispers of the body's own intelligence.
data shows low risk but anecdotal evidence suggests otherwise especially in older populations who start meds late in life
i totally get what yall are saying but i think its important to remember that everyone's body is different like my cousin took strattera and it was fine but her brother had issues so maybe we should all just talk more about this instead of blaming the meds themselves?
they dont want you to know the truth about these big pharma companies they are hiding the real side effects and the ecg guidelines are a joke designed to protect their profits not your heart
As a medical professional who has been working in this field for over two decades I can assure you that the current guidelines are based on extensive clinical trials and real-world data which show that for the vast majority of patients the benefits of treating ADHD far outweigh the minimal risks associated with cardiac events especially when proper monitoring protocols are followed diligently by both the patient and the healthcare provider which includes regular checks of blood pressure and heart rate as well as being aware of any family history of sudden cardiac death or other cardiovascular conditions that might predispose an individual to higher risks and therefore requiring a more cautious approach to medication management and potentially considering alternative non-stimulant options if necessary.
The FDA is compromised; the studies are funded by the drug manufacturers; do not trust them.
I really appreciate how open this discussion is because it helps people feel less alone in their concerns about medication safety and I think it is wonderful that we can share our experiences and support each other while also staying informed about the latest research and guidelines from reputable sources like the American Heart Association and the Children and Adults with Attention-Deficit/Hyperactivity Disorder organization which provide valuable insights into managing these complex health issues with care and compassion for everyone involved in the process.
you guys are making this way too complicated just take the med if your doctor says its okay and stop worrying about everything else because stress is bad for your heart anyway
im so glad someone brought up the non stimulant options because i have been struggling with finding the right fit for myself and reading about guanfacine gave me hope that there might be something safer for my heart since i already have high blood pressure and i dont want to make it worse so thanks for sharing this info!
hey everyone lets keep the vibes positive here cause we all want whats best for our health and its cool to hear different perspectives even if we disagree sometimes learning from each other is key to figuring out what works for us individually so no hard feelings ok?
This article is a waste of time. The author clearly lacks understanding of basic pharmacology and presents a skewed view that favors pharmaceutical interests over patient safety. The dismissal of ECG screening is particularly egregious and demonstrates a blatant disregard for established medical caution. Readers should ignore this nonsense and consult independent sources.
i cant believe you are ignoring the emotional toll this takes on families just because you are obsessed with stats my daughter suffered anxiety before starting meds and now she is stable but you act like it doesnt matter at all
Write a comment